
Urticaria can have a wide spectrum of presentations and subtypes. Urticaria is differentiated based upon its duration, with acute urticaria lasting for less than 6 weeks and chronic urticaria lasting for a longer time. Acute urticaria is more frequent, affecting about 20% of all people during their lifetime.
Chronic urticaria can be further classified into spontaneous (where wheals appear out of the blue without the need for an external trigger) and inducible forms. Other factors like stress, medications, infections, and others can worsen symptoms; however, they are not necessary for symptoms to appear.
On the other hand, patients with chronic inducible urticaria only have wheals when exposed to a specific trigger. Chronic Inducible urticaria is divided into physical urticaria and non-physical urticaria. Physical urticaria constitutes the largest group of chronic inducible urticaria. It is induced by a physical stimulus on the skin such as pressure, cold, heat, light and vibration. The distribution of wheals is localized to the site exposed to the trigger. The areas not exposed to the trigger are free of symptoms. The most common forms of inducible urticaria include symptomatic dermographism and cold urticaria. Cholinergic urticaria, contact urticaria and aquagenic urticaria are non-physical forms of chronic inducible urticaria. Cholinergic urticaria develops when wheals are brought about due to a rise in body temperature like a hot bath, exercise etc.
Chronic spontaneous urticaria constitutes the bulk of patients with chronic urticaria, while chronic inducible urticaria is less frequent. Patients with chronic spontaneous urticaria can also have associated inducible urticaria and vice versa.
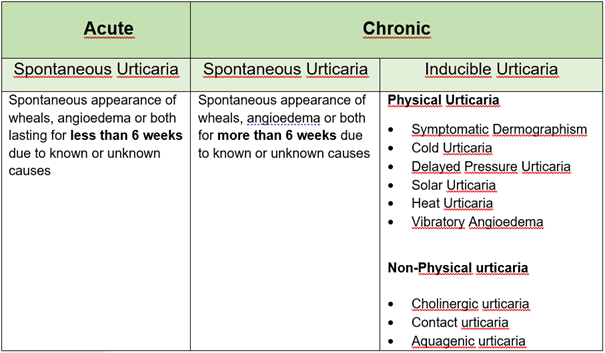

Chronic spontaneous urticaria is characterized by spontaneous (out of the blue) occurrence of itchy wheals, angioedema, or both, daily or for most of the days of the week for more than 6 weeks. This type of urticaria can take months or several years to resolve. Chronic urticaria can be a nuisance with a significant effect on the quality of life; however, it is not life-threatening.
TRIGGERS AND CAUSES
Urticaria or hives occur secondary to the activation of certain cells in the body’s immune system known as mast cells. Mast cells are commonly present in the skin, gastrointestinal and respiratory tract. In chronic urticaria, mast cell activation in the skin is triggered by the production of antibodies against the body’s own substances. Chemicals present in the mast cells like histamines are released into the skin, which can cause irritation of nerve endings resulting in localized itching. In addition, blood vessels expand and leak fluid, leading to redness and swelling. Chronic spontaneous urticaria is almost never allergic in origin. Various factors can trigger or worsen symptoms but are not the cause of urticaria itself. These include infections, medications like pain killers (aspirin, diclofenac, ibuprofen), stress, food like histamine rich foods, food additives like preservatives, color etc. Food induced worsening of symptoms are due to intolerance, and food allergy is rarely a cause of chronic urticaria. In most cases, no underlying cause can be determined.
TESTING
The diagnosis of chronic urticaria is based on symptoms, and further testing is not usually warranted. Basic tests may be done to determine the nature of the disease, especially in the presence of associated systemic symptoms, to rule out severe allergic reactions/anaphylaxis. Allergy testing for food is not indicated in patients with chronic spontaneous urticaria unless history suggests the immediate onset and recurrence of symptoms after a particular food.
TREATMENT
There is no cure for chronic urticaria at the current time, but symptoms can be controlled in most patients. The main aim of treatment is complete control over symptoms. The main treatment for chronic urticaria are antihistamines which are anti-allergy medicines. Non- sedating antihistamines (2nd generation antihistamines) are recommended, and dosage can be increased up to a maximum of 4 times the dose if symptoms are not controlled on single dosing. Biologic agents like omalizumab or immunosuppressive medications are added if antihistamines do not relieve symptoms. Although corticosteroids may be used for a short time during severe flares, steroids should not be used for long. If specific triggers like medications or food are identified, these should be avoided.
 Symptomatic dermographism is the most common type of physical urticaria characterized by the development of itching or burning sensation, wheals which are brought about by applying a sheer force on the skin like rubbing, firm stroking, scratching or scrubbing. It manifests as though someone has been writing of the skin. Itchy wheals appear within 5 minutes following the trigger and can last for 30 minutes or more. Symptoms can become worse at night and with friction. It is important to note that the skin manifestations never occur spontaneously and appear only at the sites where the stimulus is applied. Symptomatic dermographism should be differentiated from simple dermographism, where wheals without itching appear after firm stroking of the skin.
Symptomatic dermographism is the most common type of physical urticaria characterized by the development of itching or burning sensation, wheals which are brought about by applying a sheer force on the skin like rubbing, firm stroking, scratching or scrubbing. It manifests as though someone has been writing of the skin. Itchy wheals appear within 5 minutes following the trigger and can last for 30 minutes or more. Symptoms can become worse at night and with friction. It is important to note that the skin manifestations never occur spontaneously and appear only at the sites where the stimulus is applied. Symptomatic dermographism should be differentiated from simple dermographism, where wheals without itching appear after firm stroking of the skin.
TRIGGERS AND CAUSES
The cause for symptomatic dermographism is not known. Symptoms are triggered by physical stimuli on the skin like rubbing, scratching, pressure etc.
TESTING
Symptomatic dermographism can be identified through a detailed medical history and reviewing photos of wheals. Patients report the appearance of striped wheals following scratching, rubbing or pressure. The diagnosis can be confirmed by provocation testing using a wooden spatula or specialized instruments like dermographometers (Fric test). Firm pressure is applied to the skin in a stroking motion. The appearance of pruritic wheals within 10 minutes after provocation is considered positive for symptomatic dermographism. A wheal response without itching indicates simple dermographism.
TREATMENT
The management of symptomatic dermographism involves the avoidance of trigger stimuli as far as possible, including the avoidance of tight clothing, removal of tags etc. Symptoms can be controlled by the regular use of certain medications. The most recommended medications are the daily administration of a single dose of non-sedating antihistamines (anti-allergy medicines). If symptoms are not controlled on the daily administration, the dose can be increased up to four times the regular dose. Other drugs like omalizumab may be added if sufficient relief is not obtained.
Your doctor can give you more information on the available options.
 Cold urticaria is characterized by the appearance of itchy wheals, angioedema or both on skin contact with cold objects, liquids, or air. Cold urticaria is the second most common type of physical urticaria. Wheals and angioedema occur within minutes of exposure and is limited to the exposed areas of the skin; however, prolonged, extensive cold exposure (e.g., swimming in cold water) can trigger severe systemic reactions/anaphylaxis (Shortness of breath, drop in blood pressure, loss of consciousness, choking sensation etc.). Each patient has a temperature level (threshold) below which the symptoms are triggered. Temperature above this level does not trigger the onset of wheals. The higher the temperature threshold, the more frequent will the occurrence of wheals on cold exposure.
Cold urticaria is characterized by the appearance of itchy wheals, angioedema or both on skin contact with cold objects, liquids, or air. Cold urticaria is the second most common type of physical urticaria. Wheals and angioedema occur within minutes of exposure and is limited to the exposed areas of the skin; however, prolonged, extensive cold exposure (e.g., swimming in cold water) can trigger severe systemic reactions/anaphylaxis (Shortness of breath, drop in blood pressure, loss of consciousness, choking sensation etc.). Each patient has a temperature level (threshold) below which the symptoms are triggered. Temperature above this level does not trigger the onset of wheals. The higher the temperature threshold, the more frequent will the occurrence of wheals on cold exposure.
TRIGGERS AND CAUSES
The cause for the development of cold urticaria has not been determined. Symptoms are triggered by exposure to cold objects, liquids, or air.
TESTING
The diagnosis of cold urticaria is suggested by a typical history and confirmed by provocation testing. Provocation testing involves the application of a cold object on the skin. The ice cube test involves the application of a plastic bag containing an ice cube in a small amount of water against the skin for 5 minutes. The development of wheal within 10 minutes after removal is considered positive. Electronic testing devices like the Temptest available in some centers can be used for provocation testing to identify the temperature level (threshold) at which the symptoms occur and how long from exposure to cold the wheals appear.
TREATMENT
Management of cold urticaria includes avoiding cold exposure, wearing warm clothing, gloves, caps, scarves in cold temperatures. High-risk situations like exposure to cold baths, swimming, cold foods, beverages etc., should be avoided. Complete avoidance of cold exposure may be difficult. Medications can help to raise the tolerance level of cold exposure. A single daily dose of non-sedating antihistamines is recommended in patients who have frequent symptoms. Up-dosing to four times, the regular dose can be considered if the symptoms are not controlled. Other drugs like omalizumab may be added if sufficient relief is not obtained. In patients who develop severe systemic reactions/ anaphylaxis (Shortness of breath, drop in blood pressure, loss of consciousness, choking sensation etc.) following cold exposure, carrying an adrenaline auto-injector (Epipen) for emergency use may be warranted.
Your doctor can give you more information on the available options.
 Solar urticaria is a rare type of physical urticaria. In solar urticaria, itchy wheals appear within a few minutes after exposure to direct sunlight. Parts of the skin not exposed are usually unaffected. Exposure of areas of skin to sunlight through light clothes and glass can also trigger wheals as these do not completely obstruct UV rays and visible light. The severity of symptoms can increase with the intensity of sun exposure.
Solar urticaria is a rare type of physical urticaria. In solar urticaria, itchy wheals appear within a few minutes after exposure to direct sunlight. Parts of the skin not exposed are usually unaffected. Exposure of areas of skin to sunlight through light clothes and glass can also trigger wheals as these do not completely obstruct UV rays and visible light. The severity of symptoms can increase with the intensity of sun exposure.
TRIGGERS AND CAUSES
The cause for the development of solar urticaria is not clearly understood. Symptoms are triggered by exposure to direct sunlight.
Diagnosis of solar urticaria is made based on patient history and provocation testing. A simple test is the exposure of a small area of the skin to direct sunlight. A more formal evaluation is done by exposing different skin areas to different wavelengths of light (UV-A and UV-B) by phototesting. Sunscreens and photoactive medications should be avoided before photo testing. The test is considered positive if a wheal appears at the site of exposure within 10 minutes. Wheals usually subside within 1-2 hours.
TREATMENT
Patients with solar urticaria should avoid exposure to direct sunlight, wear protective clothing and use high protection sunscreens. Treatment with non-sedating antihistamines can help to control the symptoms. If symptoms are not controlled on the maximum dose of antihistamines, other drugs like omalizumab may be added.
Your doctor can give you more information on the available options.
 Delayed pressure urticaria is a subtype of physical urticaria characterized by recurrent redness and painful swelling that appears after pressure stimulus to the skin. Symptoms usually appear 4 to 6 hours after the stimulus but may occur within 30 minutes. A prominent swelling can last up to 72 hrs. Delayed pressure urticaria is generally uncommon, but it ranks third in frequency among the physical urticarias.
Delayed pressure urticaria is a subtype of physical urticaria characterized by recurrent redness and painful swelling that appears after pressure stimulus to the skin. Symptoms usually appear 4 to 6 hours after the stimulus but may occur within 30 minutes. A prominent swelling can last up to 72 hrs. Delayed pressure urticaria is generally uncommon, but it ranks third in frequency among the physical urticarias.
It can co-exist with chronic spontaneous urticaria or other types of physical urticarias. It should be differentiated from symptomatic dermographism, where the wheals appear within minutes of exposure to the pressure stimulus.
TRIGGERS
The activities that typically trigger symptoms include wearing tight clothes or shoes (affecting constricted areas), sitting on a hard surface, riding a bicycle, or standing for prolonged periods, strenuous walking (affecting the soles and feet), carrying heavy bags (affecting the palms, hands, shoulders), compression against a pillow (affecting the face).
TESTING
Patient history alone can provide adequate clues for diagnosis. Provocation testing is performed by applying sustained pressure to the skin; a common method is a sandbag test which is performed by hanging a weight from the shoulder, thigh, or forearm for 15 minutes and then observing for symptoms over the next 24hrs. The delayed appearance (approximately 6 hours) of redness and swelling at the site is considered a positive result. This is usually not associated with itching but rather a painful or burning sensation.
TREATMENT
The treatment of delayed pressure urticaria is a challenge. Initial management includes the avoidance of triggers like tight-fitting clothes, shoes, or modification of triggers (e.g., broadening the straps of bags). Although antihistamines are a first-line treatment with higher than standard doses if needed, the disease is usually resistant to antihistamines.
Your doctor can give you more information on the available options.
Heat urticaria is an uncommon form of urticaria characterized by the development of wheals, itchiness within minutes after local heat exposure to the skin (hot water or hot air). Heat urticaria should be differentiated from solar urticaria, especially when symptoms appear in the summer. In solar urticaria, only areas of the skin exposed to sunlight are involved whereas in the case of heat, urticaria skin under clothing may also be involved. Diagnosis of heat urticaria can be made by applying a test tube of hot water on the skin for 4 to 5 minutes. The test is considered positive if a wheal develops at the site after removal within 10 minutes. Temptests available in some centers can also be used for provocation testing. Non-sedating antihistamines may help to control symptoms.

Cholinergic urticaria manifests with the appearance of characteristic itchy wheals triggered by an active or passive rise in body temperature following body heating, exercise, sweating, hot baths, strong emotions etc. These patients typically develop tiny wheals surrounded by a large area of redness, frequently involving the trunk and extremities. Symptoms usually last for 15-60 minutes. Rarely patients can also have associated angioedema (swelling of the deeper skin) or systemic symptoms (Shortness of breath, drop in blood pressure, loss of consciousness, choking sensation etc.).
TRIGGERS AND CAUSES
Symptoms of cholinergic urticaria are triggered by heating, exertion, sweating, hot baths, strong emotions (excitement or fear) or eating spicy foods, unlike chronic spontaneous urticaria, where wheals appear out of the blue.
TESTING
A diagnosis of cholinergic urticaria is based on clinical presentation. Provocation testing is done to confirm the diagnosis. Moderate exercise is carried out using a stationary bike or treadmill. The test is positive if wheals appear within 10 minutes of the exercise challenge.
Another option is a passive heat challenge which can also help to differentiate cholinergic urticaria from exercise-induced anaphylaxis. This involves non-exertional elevation of the patient’s core body temperature by placing one or both arms in a hot water bath (44°C) until a rise in body temperature of at least 0.7°C is achieved. The appearance of generalized urticaria indicates cholinergic urticaria.
TREATMENT
Identification and avoidance of the triggers are crucial for managing cholinergic urticaria but may not always be possible. Non-sedating antihistamines with up-dosing in patients not responding to standard dose is effective in some patients. Other drugs like omalizumab may be added if sufficient relief is not obtained with the maximum dose of antihistamines. In patients who develop severe systemic reactions/anaphylaxis (Shortness of breath, drop in blood pressure, loss of consciousness, choking sensation etc.), carryingan adrenaline auto-injector (Epipen) for emergency use may be warranted.
Your doctor can give you more information on the available options.